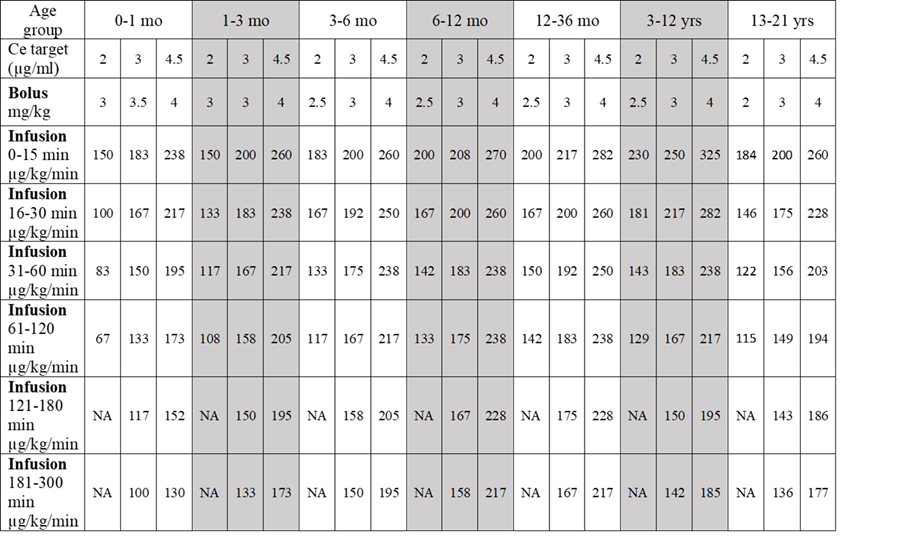
Propofol dosing for pediatric age groups
After a sevoflurane mask induction, the bolus dose should be infused over minutes — allowing the sevoflurane level to decrease to prevent hypotension.
Educational reference only. Verify all dosing against your institution's protocols, current drug references, and the individual patient.
PALNET · pedseeg.com · Smart-phone reference tables (June 2026)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}